
Surgical Options
When thinking about bariatric surgery, most literature reflects that there are two broad classes of procedures to consider: “restrictive” and “malabsorptive”. “Restrictive” bariatric surgeries limit the amount of food that can be consumed at one time. “Malabsorptive” bariatric surgeries prevent the absorption of a significant amount of calories consumed (but also nutrients, vitamins, etc.). There is actually much more to these categories than this simple two-type categorization. Let us expand on this a bit. If we look up the definition of the word “restrict” from Collins English Dictionary, it says: to confine or keep within certain often specified limits or selected bounds. In bariatric surgery, the certain specified limit is the size of the new stomach or “pouch” and the selected bounds are the lower esophageal sphincter above, and the outlet below. The outlet for a Lap-Band or other band is the opening at the band site. For a sleeve gastrectomy, the outlet is the pylorus, for the Gastric Bypass, the outlet is the anastamotic opening. We like to simplify it further by reserving the term “restrictive” for procedures with a “fixed” outlet. For all intents and purposes, even though the Lap-Band is adjustable, it is a “fixed” outlet restrictive procedure, because, once the adjustment is completed, the patient has to live with the fixed outlet size that they have between adjustments. The gastric bypass pouch outlet is the anastamosis. If this outlet is small enough to create a boundary for food passage, then it produces the restrictive element. If you band a sleeve gastrectomy, or if you create a sleeve that contains a segment that is small enough to prevent the passage of food (of certain size or viscosity), then you create a fixed outlet that is restrictive. It is our opinion that a functional pylorus does not serve well as a fixed point of restriction because it is dynamic, and can open and close variably in response to the foods eaten and other factors. As such, we refer to the performance of sleeve gastrectomy (without band and using a bougie >46) as “non-restrictive”. We like to refer to this as a “capacity reduction” procedure because although the pylorus does serve as a boundary to limit (as per the definition of restriction), it is dynamic, so that when the pylorus relaxes, the restriction is relieved in an active and dynamic manner (unlike the adjustable Lap-Band(R)). So in general, with larger bougie Sleeve Gastrectomy procedures that are not banded, you see fewer “restrictive” side effects such as nausea and vomiting. The increased meal size and meal tolerance, though, can increase the risk of weight gain or failure of weight loss. We separate our procedures, therefore, into three categories: 1. Restrictive (band or bypass), 2. Capacity Reduction (sleeve without band), and 3. Malabsorptive (Biliopancreatic Diversion with or without Duodenal Switch, Scopinaro Procedure). Keep in mind that the BPD-DS does also involve a capacity reduction 90 cc sleeve gastrectomy, and the gastric bypass does involve the dumping syndrome which produces a state of relative sweet intolerance.
Dr. Elariny and his associates perform a broad spectrum of bariatric procedures, primarily via minimally invasive (laparoscopic) and robotic approaches. These minimally invasive approaches mean that a few small incisions are made in the abdomen (0.5-2.0cm each), and the surgeon uses long, thin instruments to perform the procedure while a small, thin camera allows the surgeon to see as (s)he performs the operation.
We perform the Lap-Band, sleeve gastrectomy, vertical banded gastroplasty with sleeve gastrectomy, gastric bypass, and biliopancreatic diversion with duodenal switch. We also perform a variety of revisional bariatric procedures.
Please attend one of our seminars or webinars for more information about how to make sense of the different procedures that are available, and how to best achieve your personal goals. Although you will find plenty of information about each procedure in the following sections, these are by no means exhaustive reviews or definitive statements on the topics. Please contact us with any questions, concerns, or comments and we will be glad to assist you in any way that we can. Remember that any surgery comes with associated risks, but you must ultimately weigh these surgical risks against the risks that come to your health from being overweight. We can help you make sense of all this information so do not hesitate to call. We are here to assist you on your path to health and well being.
Lap Band
Gastric banding procedures, including the LAP-BAND® System and the REALIZE® Adjustable Gastric Band, reduce the stomach’s capacity for food intake, restricting the amount of food a patient is able to eat at one time. Ideally, the patient should feel full faster and stay full longer.
There is no use of surgical staples, no resection of any part of the stomach, or any cutting or manipulation of the intestines. In the procedure, the Band is placed around the uppermost part of the stomach, effectively dividing the stomach into a small upper segment, or “pouch”, and a larger lower stomach. The small upper pouch can only hold a few ounces (1/2 cup) of food (thus, the restriction).
These Bands are made of biocompatible materials that are meant to stay in the body without causing harm. The side of the Band that fits against the stomach is lined with a soft, adjustable balloon. After the surgery (in an outpatient office setting), saline can be delivered to the balloon by accessing a small port that sits on the patient’s abdominal wall under the skin with a special needle to control the band tightness. The degree of band tightness affects how much food someone can eat during a meal and the length of time it takes for food to empty from the upper pouch. When the band is adjusted to the proper tightness, the patient should feel full sooner, helping him or her eat less food, and consume less calories.
Of all of the bariatric procedures performed, the gastric banding procedures are the “simplest” procedures surgically, with the lowest immediate surgical risk and the least amount of time under anesthesia. Patients require the least amount of additional multivitamins in the long run, with protein needs obtained by food primarily; protein shakes and supplements may not be needed. Furthermore, this procedure is “reversible”, in that the band can be removed—but how important should this be in a patient’s decision making? There is also a low long-term malnutrition or vitamin deficiency risk. However, these facts must be evaluated against the overall efficacy of the procedure itself.
Risks/complications associated with gastric banding include:
- Band erosion (The band wears away the wall of the stomach)
- Band slippage (The band migrates allowing the lower stomach to slip through it, potentially causing obstruction and inability to eat)
- Port flipping or displacement
- Tubing-related complications (port disconnection, tubing crack)
- Band leak
- Esophageal spasm, or Esophageal Dilation (Mega-Esophagus)
- Gastroesophageal reflux disease (GERD)
- Inflammation of the esophagus or stomach
- Port-site infection
- Wound complications
In considering studies of effectiveness of bariatric surgery, gastric banding has been shown to have the lowest percent of excess body weight lost of all procedures performed (35-45% EBW at one year and 45-55% EBW at 3 years). It also has the highest overall failure rate (as much as 40% of people are unsuccessful at maintaining weight loss), particularly in patients who snack a lot or get a lot of their calories from sweets. Furthermore, resolution of comorbidities depends primarily on successful weight loss versus some of the other procedures in which there is significant improvement in certain comordid conditions (e.g., diabetes, hypertension) within days of the surgery.
Sleeve Gastrectomy (and Vertical Banded Gastroplasty with Sleeve Gastrectomy)
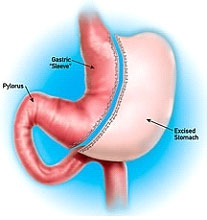 In the sleeve gastrectomy, 80-85% of the capacity of the stomach is removed from the body, fashioning the stomach into a narrow, tubular shape similar to that of a banana. Many consider the Sleeve Gastrectomy to be a restrictive procedure. However, this conclusion of category can only be made if we understand and consider the definition of restrictive. The sleeve gastrectomy is primarily a restrictive procedure, limiting the amount of food a patient can consume at one time. Ultimately, this amounts to about a 2 ounce meal.
In the sleeve gastrectomy, 80-85% of the capacity of the stomach is removed from the body, fashioning the stomach into a narrow, tubular shape similar to that of a banana. Many consider the Sleeve Gastrectomy to be a restrictive procedure. However, this conclusion of category can only be made if we understand and consider the definition of restrictive. The sleeve gastrectomy is primarily a restrictive procedure, limiting the amount of food a patient can consume at one time. Ultimately, this amounts to about a 2 ounce meal.
Under Construction…..
 Linkdin
Linkdin